Carpal tunnel syndrome in a Maryland Workers Compensation case
The nerves in your body are responsible for transmitting messages to and from your brain. If the nerves are compressed, damaged, or irritated, numbness can occur. Finger numbness may affect your ability to pick things up. You may feel clumsy and as if you’ve lost strength in your hands. Hand numbness is usually caused by damage, irritation or compression of one of the nerves or a branch of one of the nerves in your arm and wrist.

Symptoms
Carpal tunnel syndrome symptoms usually start gradually. The first symptoms often include numbness or tingling in your thumb, index and middle fingers that comes and goes.
Carpal tunnel syndrome may also cause discomfort in your wrist and the palm of your hand. Common carpal tunnel syndrome symptoms include:
- Tingling or numbness. You may experience tingling and numbness in your fingers or hand. Usually the thumb and index, middle or ring fingers are affected, but not your little finger. Sometimes there is a sensation like an electric shock in these fingers.
The sensation may travel from your wrist up your arm. These symptoms often occur while holding a steering wheel, phone or newspaper. The sensation may wake you from sleep.
Many people “shake out” their hands to try to relieve their symptoms. The numb feeling may become constant over time.
Weakness. You may experience weakness in your hand and a tendency to drop objects. This may be due to the numbness in your hand or weakness of the thumb’s pinching muscles, which are also controlled by the median nerve.
Carpal tunnel elicits numbness in the distribution of the median nerve, nocturnal symptoms, thenar muscle weakness/atrophy, positive Tinel’s sign at the carpal tunnel, and abnormal sensory testing such as two-point discrimination Electrodiagnostic testing (electromyography and nerve conduction velocity) can objectively verify the median nerve dysfunction. Normal nerve conduction studies, however, do not exclude the diagnosis of CTS. Clinical assessment by history taking and physical examination can support a diagnosis of CTS. If clinical suspicion of CTS is high, treatment should be initiated despite normal electrodiagnostic testing.

Although widely used, the presence of a positive Phalen test, Tinel sign, Flick sign, or upper limb nerve test alone is not sufficient for diagnosis.
- Phalen’s maneuver is performed by flexing the wrist gently as far as possible, then holding this position and awaiting symptoms. A positive test is one that results in numbness in the median nerve distribution when holding the wrist in acute flexion position within 60 seconds. The quicker the numbness starts, the more advanced the condition. Phalen’s sign is defined as pain and/or paresthesia in the median-innervated fingers with one minute of wrist flexion.
- Tinel’s sign is a classic test to detect median nerve irritation. Tinel’s sign is performed by lightly tapping the skin over the Flexor Retinaculum to elicit a sensation of tingling or “pins and needles” in the median nerve distribution. Tinel’s sign (pain and/or paresthesia of the median-innervated fingers with percussion over the median nerve), depending on the study, has 38–100% sensitivity and 55–100% specificity for the diagnosis of CTS.[6]
- Durkan Test, carpal compression test, or applying firm pressure to the palm over the nerve for up to 30 seconds to elicit symptoms has also been proposed.
- Hand Elevation Test The hand elevation test is performed by lifting both hands above the head, and if symptoms are reproduced in the median nerve distribution within 2 minutes, considered positive. The hand elevation test has higher sensitivity and specificity than Tinel’s test, Phalen’s test, and carpal compression test. Chi-square statistical analysis has shown the hand elevation test to be as effective, if not better than, Tinel’s test, Phalen’s test, and carpal compression test.
As a note, a patient with true carpal tunnel syndrome (entrapment of the median nerve within the carpal tunnel) will not have any sensory loss over the thenar eminence (bulge of muscles in the palm of hand and at the base of the thumb). This is because the palmar branch of the median nerve, which innervates that area of the palm, branches off of the median nerve and passes over the carpal tunnel. This feature of the median nerve can help separate carpal tunnel syndrome from thoracic outlet syndrome, or pronator teres syndrome.
Other conditions may also be misdiagnosed as carpal tunnel syndrome. Thus, if history and physical examination suggest CTS, patients will sometimes be tested electro-diagnostically with nerve conduction tests and electromyography. The goal of electrodiagnostic testing is to compare the speed of conduction in the median nerve with conduction in other nerves supplying the hand. When the median nerve is compressed, as in CTS, it will conduct more slowly than normal and more slowly than other nerves. However, normal electrodiagnostic studies do not preclude the presence of carpal tunnel syndrome. Carpal tunnel syndrome with normal electrodiagnostic tests is very, very mild at worst.
Carpal tunnel injuries in a Maryland Workers Compensation claim create numerous issues that often result in insurance companies refusing to pay for necessary treatment unless ordered to do so by the Maryland Workers Compensation Commission. Issues include the following:
- Does the employee have carpal tunnel syndrome? Carpal tunnel syndrome can be difficult to diagnose. Diagnosis of carpal tunnel syndrome. A combination of described symptoms, clinical findings, and electrophysiological testing may be used. CTS work up is the most common referral to the electrodiagnostic lab. Historically, diagnosis has been made with the combination of a thorough history and physical examination in conjunction with the use of electrodiagnostic (EDX) testing for confirmation. Additionally, evolving technology has included the use of ultrasonography in the diagnosis of CTS.
- What caused the carpal tunnel syndrome? For Workers compensation purposes, carpal tunnel as a worker’s compensation claim is either due to an accident such as wear you fracture your wrist on the job and develop carpal tunnel syndrome or more frequently due to an occupational disease. An occupational disease carpal tunnel case involves carpal tunnel that develops over a long period of time due to repetitive motion at work and it must be inherent in the type of work you do. In order to have a successful occupational disease claim you will need the following:
- Doing repetitive work all day with no brakes other than lunch or an occasional break. If you work 8 hours per day but only do the repetitive part for two of those hours with frequent changes of job in between that will unlikely be sufficient, since it is the repetitive nature of eight hours per day, 5 days a week for months that makes the claim easier to make.
- It usually takes months to develop
- It must be inherent in your job. There needs to be some proof that statistically shows that the type of work you do has a higher rate of carpal tunnel cases than the normal population. Proof of co-employees with the same condition is helpful. Workplace factors. It’s possible that working with vibrating tools or on an assembly line that requires prolonged or repetitive flexing of the wrist may create harmful pressure on the median nerve or worsen existing nerve damage. Types of work that are associated include computer work, work with vibrating tools, and work that requires a strong grip.
- Carpal tunnel syndrome is provoked by repetitive movement and manipulating activities and that the exposure can be cumulative. It has also been stated that symptoms are commonly exacerbated by forceful and repetitive use of the hand and wrists in industrial occupations. Job tasks that involve highly repetitive manual acts or specific wrist postures were associated with incidents of CTS.
- Unlike other workers compensation cases an occupational disease carpal tunnel case can- not be an aggravation of an underlying medical condition. If you are already having numbness and tingling in your hand before you start a job and the job makes it worse this will normally not be accepted as an occupational disease.
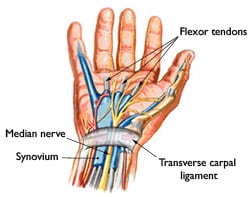
- Carpal tunnel syndrome is caused by pressure on the median nerve. The median nerve runs from your forearm through a passageway in your wrist (carpal tunnel) to your hand. It provides sensation to the palm side of your thumb and fingers, except the little finger. It also provides nerve signals to move the muscles around the base of your thumb (motor function). Anything that squeezes or irritates the median nerve in the carpal tunnel space may lead to carpal tunnel syndrome.
- Carpal tunnel syndrome can be caused by many different methods that are not work related. Because there is a disagreement in the medical community as to whether carpal tunnel can be induced by repetitive work activity the Maryland Workers Compensation Commission normally rules as follows. If any of the below conditions are part of your medical history the workers compensation commission is likely to deny your claim. If these conditions do not exist and you describe repetitive activity at work, then the Maryland Workers Compensation Commission normally rules in favor of an occupational disease.
- Anatomic factors. A wrist fracture or dislocation, or arthritis that deforms the small bones in the wrist, can alter the space within the carpal tunnel and put pressure on the median nerve.
- A wrist fracture can narrow the carpal tunnel and irritate the nerve.
- People with smaller carpal tunnels may be more likely to have carpal tunnel syndrome.
- Sex. Carpal tunnel syndrome is generally more common in women. This may be because the carpal tunnel area is relatively smaller in women than in men. Women who have carpal tunnel syndrome may also have smaller carpal tunnels than women who don’t have the condition.
- Obesity. Being obese is a significant risk factor for carpal tunnel syndrome.
- Alterations in the balance of body fluids. Fluid retention may increase the pressure within your carpal tunnel, irritating the median nerve. This is common during pregnancy and menopause. Carpal tunnel syndrome associated with pregnancy generally resolves on its own after pregnancy.
Carpal Tunnel syndrome can often be mistaken for other medical conditions.
- Carpal tunnel syndrome can be similar to C6 radiculopathy because both are typically felt on the thumb side of the hand and wrist. However, C6 radiculopathy is likely to be accompanied by other symptoms higher up the arm, such as weakness in the bicep. In contrast, carpal tunnel syndrome might involve weakness in the thumb.
- Rheumatoid Arthritis
While Rheumatoid arthritisis an autoimmune disease that can cause pain, tingling, and/or numbness in the hands, it usually is felt in both hands. So, if a certain joint in the left hand is affected, then that same joint in the right hand is also probably affected. See Cervical radiculopathy, herniated or bulging disc in neck. Cervical radiculopathy, however, is typically only felt on one side of the body. If rheumatoid arthritis progresses long enough, the swelling in the wrist can actually cause carpal tunnel syndrome. - Nerve dysfunction—either due to damage or disease—is known as neuropathy. Typically, neuropathy involves numbness or weakness in one or more parts of the body.
- Diabetes.A condition called diabetic neuropathy can lead to nerve damage in the feet as well as the hands. The feet are usually the first to have numbness. If diabetes progresses or isn’t managed well with diet and/or medications, various complications can develop. One of the more serious complications of diabetes is neuropathy. For people who have diabetes, these symptoms of tingling and numbness usually start in the feet, but they can also occur in the hands.
- Vitamin B12 deficiency.Some people don’t get enough vitamin B12, whether through gaps in their diet, inability to naturally absorb enough of it, or as a side effect of a medical condition or treatment. Vitamin B12 is critical for nerve health, so low levels can harm the nerves and result in numbness and/or weakness.
- Alcohol abuse. Excessive amounts of alcohol can harm nerves. The manner in which the nerves are damaged by alcohol isn’t always known, but experts suspect that multiple factors could be at work, including increased difficulties with nutrient absorption and associated poor diet. Someone with a long-term alcohol problem could also be at increased risk for a vitamin B12 deficiency as mentioned above.
- traumatic injury to the hand, such as a broken bone or deep cut, could lead to nerve damage that leaves part of the hand painful, numb, tingling, and/or weak.
- Cervical Radiculopathy-This occurs when a nerve that leaves your neck becomes inflamed or compressed. This condition can cause numbness that’s similar to carpal tunnel syndrome. This is also known as a pinched nerve.
- Raynaud’s Disease-This condition causes the small arteries in your fingers to spasm, or open and close very fast. This can cause numbness and affect your circulation.
- Ulnar Entrapment -Carpal tunnel syndrome affects the median nerve in the arm, but ulnar nerve entrapment affects the ulnar nerve that runs on the little finger’s side of the arm. This most commonly causes numbness in the pinkie and ring fingers.
- Less common causes of finger numbness can include:
- Ganglion cyst
- Guillain-Barre syndrome
- HIV
- Lyme Disease
- Multiple Sclerosis
- side effects of medications
- Sjogren’s syndrome
- Brachial Plexus injury
- Raynaud’s disease
- Stroke
- syphilis

Treatments for carpal tunnel syndrome include:
Generally accepted treatments include: physical therapy, steroids either orally or injected locally, splinting, and surgical release of the carpal ligament. Change in activity may include avoiding activities that worsen symptoms.
- Orthopedic Surgeons recommend proceeding conservatively with a course of nonsurgical therapies before release surgery is considered. Non- surgical treatment should be tried for 2 to 7 weeks. Early surgery with carpal tunnel release is indicated where there is evidence of median nerve denervation or a person elects to proceed directly to surgical treatment.
- Splints- Many health professionals suggest that, for the best results, one should wear braces at night and, if possible, during the activity primarily causing stress on the wrists.
- Current recommendations generally don’t suggest immobilizing braces, but instead activity modification and non-steroidal anti-inflammatory drugs as initial therapy, followed by more aggressive options or specialist referral if symptoms do not improve.
- Steroid injections can be effective for temporary relief from symptoms. This form of treatment is thought to reduce discomfort in those with CTS due to its ability to decrease median nerve swelling. The injections are done under local anesthesia This treatment is not appropriate for extended periods, however.
- Physical Therapy-One of the primary issues with physiotherapy is that it attempts to reverse (often) years of pathology inside the carpal tunnel. Practitioners caution that any physiotherapy such as myofascial release may take weeks of persistent application to effectively manage carpal tunnel syndrome.
- Change in Ergonomics of job-Pro-active ways to reduce stress on the wrists, which alleviates wrist pain and strain, involve adopting a more ergonomic work and life environment.
- Surgery-Carpal tunnel syndrome operation-Release of the transverse carpal ligament is known as “carpal tunnel release” surgery. It is recommended when there is static (constant, not just intermittent) numbness, muscle weakness, or atrophy, and when night-splinting or other conservative interventions no longer control intermittent symptoms. The surgery may be done with local anesthesia. Milder cases can be controlled for months to years, but severe cases are unrelenting symptomatically and are likely to result in surgical treatment.
For more info on Workers Comp Claims in Maryland, CLICK HERE.